

by Jeongpyo Hong
figures by Xiaomeng Han
edited by Sarah Kalinowski
A little boy is in the hospital to fix his leg. His surgeon uses spinal rods developed for adults to fix the little boy’s leg as it is the only thing that really fits. Since the rod was developed for an adult spine, its clinical safety and effectiveness in the legs of children – with considerations like the bone density and mechanical strength – remain unknown.
Medical products save people’s lives every day, and new developments in medical products improve patient treatment. However, children do not benefit from these advancements to the same degree as adults. Manufacturers are not interested in developing medical products for children, as it requires much greater investment than for adults, while the market is small. Clinical trials are the longest and most costly stage of medical product development, and they are especially challenging in children. Children are classified as a vulnerable population, so they require additional protection, and the low volume of patients lengthens the study duration and increases costs. The lack of medical products available often causes doctors to turn to off-label use of medical products in children.
What is off-label use?
Off-label use refers to the use of FDA-approved medical products for treatment beyond the approved range of diseases or populations.Throughout the FDA review process, subject matter experts review scientific evidence of the safety and efficacy of a medical product for target patient populations and diseases. Patient populations and disease contexts for which the FDA deems a medical product safe and effective are written on its labels as “usage and indications”. However, FDA-approved medical products are not available for all patients. Children need medical products to treat their diseases, but there is a dearth of medical products that are approved for pediatric use. In these cases, physicians on their own must determine whether medical products approved for other diseases or populations would be useful, effective, and safe for their patient. Due to the limited scientific evidence, physicians choose medical products largely based on the experience of other clinicians and data from adult studies, unlike approved medical products, which undergo multifaceted scientific review by the FDA (Figure 1).

Four in five prescriptions used off-label don’t have strong scientific evidence backing their use, which leads to an increased risk of resulting medical problems. Products used off-label have a 44% higher risk of adverse events than products used on-label, although off-label medical products prescribed with strong scientific evidence have similar adverse event risk with on-label use. A lack of scientific evidence contributes to the higher risk in medical products’ off-label use.
Off-label use of medications is common in pediatrics. One third of children in the hospital and up to 90% of newborns in neonatal intensive care units receive off-label prescriptions. Patients who received off-label treatment in the neonatal ICU have significantly higher adverse reactionssuch as extrapyramidal effects: involuntary movements cannot control than on-label treatment. Clinicians extrapolate from the data on drug safety and efficacy in adults to estimate their safety and efficacy in children. For example, Carvedilol (brand name: COREG) is a drug commonly prescribed for patients with heart failure, as well as pediatric cardiac patients, but its package insert states, “Effectiveness of COREG in patients younger than 18 years has not been established”.
What policies have been implemented to reduce off-label use in children?
Several policies have been introduced to mitigate the problem of off-label use in children, but their effects are limited. The Best Pharmaceuticals for Children Act (BPCA) of 2002 incentivizes companies to conduct pediatric studies by adding six months of additional exclusivity to a medicine’s patent if they do. The Pediatric Research Equity Act (PREA) of 2003 requires drug manufacturers to submit a pediatric study plan when submitting a new drug application to the FDA. Although the pediatric study is a requirement, pharmaceutical companies can sell their product without the pediatric study report if the FDA approves a deferral. With BPCA and PREA, FDA-approval of new drugs for children increased from 21.6% to 46.6%. Adolescents benefitted the most from these changes, while neonates benefited least.
The FDA’s Pediatric Device Consortia Grants program has provided funding and consultation on pediatric medical device development. Since its start in 2008, over 800 projects were assisted and 19 pediatric devices have been placed on the market. Although these policies have successfully increased pediatric medical products in the U.S. market, they are focused on new products, and there have been few changes in the use of products already in the market.
Real clinical data can help evaluate safety and efficacy
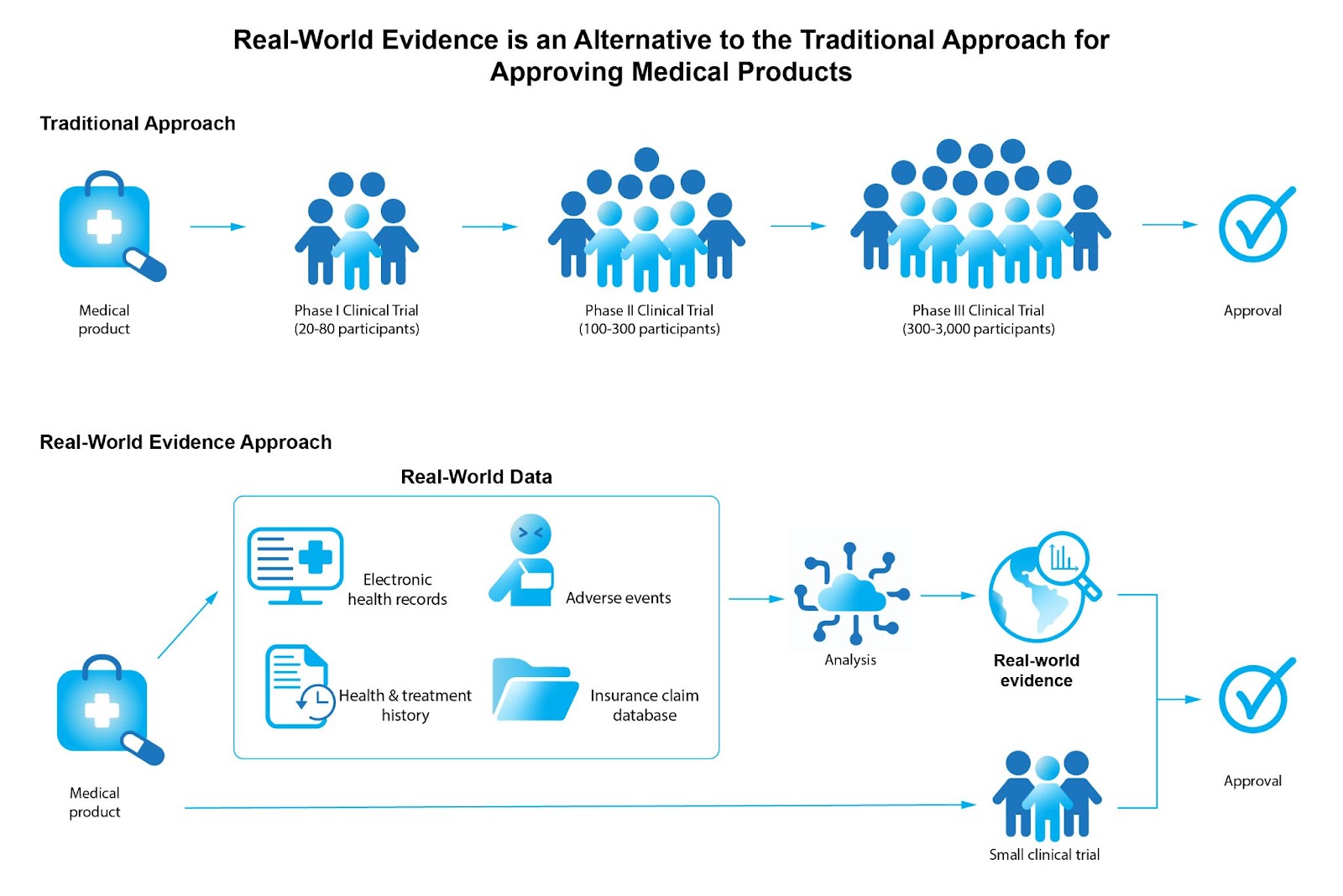
Data relating to patient health status, such as doctor’s notes stored in electronic health records, are termed “real-world data” (RWD). Clinical evaluation of RWD is called “real-world evidence” (RWE). Although RWE is useful to evaluate the safety and efficacy of medical products in real clinical settings, RWE had only been used by the FDA to monitor safety after medical products were on the market. The 21st Century Cures Act of 2016 created an RWE program in the FDA, where RWE can be used instead of clinical trials for FDA approval. As clinical trials are highly challenging when working with children, substituting RWE in place of clinical trials made pediatric medical product development easier for manufacturers.
For example, the Melody Transcatheter Pulmonary valve expanded its approved usage without a clinical trial of children by using RWE. For initial approval for use to replace a leaky valve between the heart and lungs,over 300 participants including children were required for clinical trial. To expand its approved usage fixing leaky or clogged pre-implanted valves–valve-in-valve–only 25 adults were required for the clinical trial as RWE from off-label use record could support its clinical evidence (Figure 2).
However, there are remaining challenges. RWD is still mostly used in conjunction with clinical trials to gain confidence to evaluate the response of patients who have used medical products. Even though ample RWD can be easily collected, as most hospitals use a digital system to manage patient data, the number of medical records is huge and has too many variables to analyze. Furthermore, important clinical information such as a patient’s progress or reaction after using a product are in a clinician’s notes in paragraph form, so this key information is not easily found and extracted. Modern tools in data science may allow for the analysis of these notes to draw conclusions about the efficacy of a medical product.
Real-World Evidence can be a tool to ensure safe and effective use of medical products for children.
Though there is a need for pediatric medical developments, clinical trials for children have been a major obstacle, leading to off-label use of medical products. Using RWE ordered by the 21st Century Cures Act, pharmaceutical and medical device industries can expand approved use of their products for children with significantly less investment than clinical trials. More importantly, physicians and patients can ensure the safety, efficacy, and effectiveness of medical products prescribed by using FDA-approved medical products converted from off-label use, rather than relying on an individual’s experience or limited information.
Jeongpyo Hong is a Master of Public Health graduate in Health Policy at Harvard T. H. Chan School of Public Health.
Xiaomeng Han is a graduate student in the Harvard Ph.D. Program in Neuroscience. She uses correlated light and electron microscopy to study neuronal connectivity.
Cover image by Emilian Danaila from Pixabay